

How To Prevent Re Injury Of A Jones Fracture Surgical Repair
Introduction [edit | edit source]

Stone climbing has become a professional competitive sport, many folks are being drawn to this sport with a parallel increase in the occurrence of sport-related injuries on both the natural stone and artificial walls. Information technology emphasizes on physical and mental challenges, one that often tests climber's upper and lower body flexibility, strength, endurance, agility, and balance along with mental control. It is a popular sport with the explosion in climbing gyms, bouldering venues and, bolted sports routes.
Excessive loading of the upper extremities, contorted positioning of the lower extremities, rockfall, and falling from tiptop create an elevated and diverse injury potential that's hampering feel level and quantity of participation. Injuries tin can range from acute trauma to chronic overuse injuries. Unique sport-specific injuries to the flexor tendon pulley system exist, merely the remaining Musculoskeletal conditions aren't exempt from these types of injuries.[1] Agreement the techniques of rock climbing and its injury patterns, treatments, and prevention is of import to diagnose, manage, and counsel the rock-climbing athlete.
Chance Factors [edit | edit source]
one. Age
two. Higher skill (difficulty) level
iii. high CIS (Climbing Intensity Score)
4. Poor climbing movement pattern:
- An example of climbing inefficiently with bent elbows- This increases the stress on biceps.
- Climbing with elbows in a chicken fly- This puts excessive stress on the shoulder joint and is a event of latissimus dorsi and shoulder internal rotators working too difficult.
- Likewise much wrist flexion and tin can compress the articulation and nervus in the wrist as well as pb to elbow pain.
5. Participating in lead climbing
vi. Using inadequate climbing equipment's
seven. Improper footwear- shoes that are too pocket-size and tight
8. Climbing in bad atmospheric condition condition
ix. Over-training lead to a number of overuse and traumatic injuries.
Prevalence and incidence of injuries [edit | edit source]
Studies that have estimated the prevalence of injuries associated with rock climbing vary between 10% and 81% irrespective of the cause. between 10% and l% for impact injuries, between 28% and 81% for non-touch acute trauma injuries, and between 33% to 44% for chronic overuse injuries.[2]
Machinery of Injury [edit | edit source]
Climbing in a higher place one's skill level, the weight of a climber places an extensive amount of stress non just on their fingers, but also on their wrists, elbows, and shoulders.
- Inherent within the characteristic of sport, climbers frequently bailiwick their bodies to recurrent traumatic forces, whether from throwing to succeed in holds (denoting and dead pointing) or falling from climbs (peculiarly with bouldering), which leads to either acute or overuse injuries.
- This apparent pattern of overuse injuries may be associated with the architecture of climbing walls, climbing techniques, specific training, or relative weakness of a specific grouping of muscles.
Injuries in rock climbers [edit | edit source]
Climbing-related injuries may exist categorized as:
- Impact injury acquired by the climber falling onto a climbing surface and/or basis, or an object, such equally a rock falling on to the climber.
- Non-impact injury resulting from acute trauma to the torso.
- Chronic overuse injury from repetitive climbing.
A survey conducted shows, the bulk of injuries (82%) were categorized by the respondents equally overuse injuries. Upper extremity injuries were the vast majority and deemed for 63% of all injuries. Hand overuse injuries predominated (28% of all injuries), although elbow injuries were a shut 2nd (19%). Combined upper extremity overuse injuries were mutual. Consideration of the anatomical distribution of injuries associated with rock climbing may be useful in injury prevention and in the rehabilitation of the injured climber.[3]
Themost mutual injuries seen in stone climbers are:
Upper Extremity [edit | edit source]
Sport rock climbing with it's repetitive loftier-torque movements in gaining the rise of a stone confront or wall, often in steep overhanging positions, is associated with a unique distribution and grade of upper limb injuries.[four] Injuries of the upper extremity are often among climbers.[5] They vary from light abrasions, through more than severe like SLAP Lesion, Flexor digitorum tendon pulley injury, rotator cuff tears; to bony fractures like hamate fracture and phalangeal epiphyseal stress fracture. The most often injured part of the upper extremity is the flexor digitorum tendon pulleys [vi] [7] [viii]
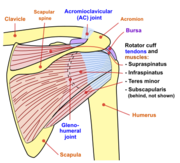
Shoulder injuries in climbing [edit | edit source]
The shoulder typically accounts for 17% of all climbing-related injuries. Sport climbers and boulders are particularly susceptible to the evolution of shoulder injuries due to prolong repetitive upper limb movements on vertical or overhanging terrain. A cross-sectional cohort study of 201 climbers found the shoulder injuries to be related to the frequency and difficulty of indoor and outdoor sport climbing and bouldering.[nine] An analysis of injury trends in sport climbing and bouldering over 4 year period constitute superior labral inductive-posterior tears and impingement of subacromial structures to be the common diagnosis in most of the climbers.
Subacromial Impingement [edit | edit source]
The unique physical demands associated with climbing, also equally a reported 33-51% incidence of shoulder injuries in these athletes is suggestive of abnormalities in scapulohumeral biomechanics [10] Clinically climbers with shoulder and arm symptoms are commonly observed with poor scapulothoracic and Glenohumeral control (Kibler et al. 2022). Scapula positioning on the thorax is important in lodge to create a stable base for shoulder movement and maintain humeral caput in the center of the glenoid. If the scapula is not moving properly, the shoulder joint will take to pick upward the slack, this puts the climber at an increased risk of impingement.
Often most of the rock climbers testify the relative weakness of shoulder external rotators (Teres small-scale and infraspinatus). These muscles are a part of a rotator cuff located on the back of the scapula. Information technology helps to stabilize the glenohumeral joint during up reaching. This muscular imbalance creates a high take a chance of shoulder impingement.
Rotator Cuff Injuries [edit | edit source]
These injuries are common in rock climbers considering of the corporeality of time they spent with their arms overhead pulling upwards their body weight. The rotator cuff provides stability for the shoulder. Information technology'south comprised of tendons that attach to the humerus, as well every bit the four major muscles that surround the shoulder complex. A weak rotator cuff and/or altered biomechanics can contribute to a tear o tendonitis. Mutual symptoms include pain, weakness on lifting heavy objects or lowering the arm, restricted range of motion, and hearing clicking or popping sound.
Physiotherapy Direction [edit | edit source]
Conservative treatment can be constructive in treating tendonitis and fractional tears. This includes relative rest, ice, anti-inflammatory medications, corticosteroid injects, and physiotherapy. The Exercise plan will focus on activating the advisable muscles during climbing, and so progressively strengthen them to better functioning and minimize the gamble of injury in the futurity.
Rotator cuff strengthening: For a shoulder, exercise to exist effective it must be functional. At that place are 2 exercises which are plant to be effective.
- Wall clock: It strengthens rotator gage muscles by simulating the action of reaching for climbing holds in varied positions.
- Looped Band Reaches: Information technology strengthens and stabilizes the shoulder in a range of movement that is required to take during climbing. How to do: Wrap a single resistance ring around the westward. Sit into a mini squat to mirror the position of the lower limb when climbing. Press outwards on the band and raise the arms overhead.
- Robber *Scapular retraction
- Windmill *Scapular retraction
- Bent over I, T, Y
- Rows
- Hanging Scapular retractions
- Pull-ups:
- Weight assisted with ring
- Shoulder width
- start or wide: This position increases the likelihood of impingement, progress to this simply the pain-free in the easier version of button-ups.
nine. External rotation with a band, weights, etc.
10. Shoulder blade repositioning- Rigid taping can be done in example of scapular dyskinesia.
If symptoms don't go away or in that location is a complete rotator cuff tear surgery may be necessary to repair the tendon. Research has shown favorable outcomes afterward an arthroscopic repair in climbers that volition allow most athletes to return to or near their pre-injury level of climbing. Thus, surgery is a valid treatment for climbers with astute traumatic tears and those with chronic tears who fail to reply to conservative treatment.[xi]
Elbow injuries [edit | edit source]
Lateral epicondylalgia (Ordinarily referred to as tennis elbow) is a very common elbow injury. This is caused by excessive forces on the lateral elbow due to increased muscle overuse of extensor forearm muscles. Symptoms include pain at the exterior of the elbow aggravated by repetitive gripping activities.
Physiotherapy Direction [edit | edit source]
Treatment may include the following:
- Relative rest
- Ice, anti-inflammatories
- Bracing (Forearm counter-strength caryatid, wrist anti-extension brace). These braces help offload the muscles that attach to the elbow, decreasing the excessive pulling on the area and allowing it to heal chop-chop.
- Unloading taping (diamond taping)
- Myofascial release techniques to the wrist extensors
- The gradual strengthening of wrist extensors (concentric and eccentric) using weights and flexibar.
- Progressive return to climbing.
*A annotation on corticosteroid injections: injection appears to take superior brusk-term outcomes even so, physiotherapy handling is more constructive in the intermediate to long-term than injection or "wait and see" lone.
Hand Injuries [edit | edit source]
Based on recent series >75% of elite and recreational sport climbers are reported to accept injuries at upper extremities, and upward to 30% of them have specific signs of flexor pulley system rupture with the loss of strength across the full range of motion of a finger, decrease Ange of move and bowstringing.[12]
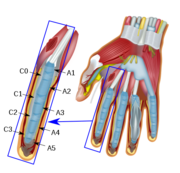
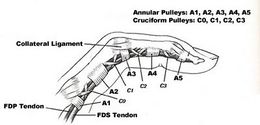
Clinically Relevant Anatomy [edit | edit source]
As shown in the film, The four- long white, rope-like structures are tendons that help in gripping and crimper of fingers. These are secured to the basic below by circular structures chosen "Pulleys". There are v pulleys on the palm side of each finger. The A2 pulley is located in the first finger of the proximal phalanx cupboard to the palm.
Annular Pulley injury [edit | edit source]

One of the most common and unique lesions occurring in the stone climbing population is the closed rupture of the flexor caster organisation of the fingers due to Closed-hand crimping . An A2 pulley strain is the nigh mutual finger injury for climbers and most oftentimes occur in the ring or eye finger. These injuries can vary from a balmy strain or a complete tear. This type of injury is strictly associated with some climbing techniques in which the whole body weight is placed on finger holds, which causes bowstringing of the flexor tendons with subsequent loss of forcefulness beyond the complete range of motion of the finger and this places three-4 times more stress on A2 pulley than at the fingertip.
Overusing full crimps weakens pulleys, making them susceptible to breaking considering of the position of A2 and A4 pulleys, along with the strength ratio of the two finger flexor tendons, a crimp position applies a strong "bowstring" tension on to them. This combined with a full maximum wrinkle of 2 tendons exerts a bowstringing (bulging) forcefulness outwards, pushing and stretching the pulleys. These forces may add upwardly to reach a betoken threshold and so a tear, strain or rupture can occur.
Grades of injury [edit | edit source]
There are four dissimilar levels of flexor pulley injuries:
- Class I: Strain
- Grade II: Partial rupture
- Grade III: Unmarried pulley rupture
- Grade Iv: Multiple pulley rupture
More often than not, class I-III are treated conservatively with initial immobilization and early functional therapy under caster protection.
- Course I-2 usually can achieve full recovery in 6 weeks, should keep protective taping for 3 months following an injury.
- Form Iii should exist immobilized in a splint for 10-14 days, protective taping for six months following an injury. Can return to gentle climbing at 6-8 errs, with full climbing at three months.
- Grade IV injuries (multiple ruptures) require surgical repair.
Clinical Presentation: [edit | edit source]
Climbers unremarkably present with pain and tenderness on the palmer aspect of a finger and an audible "pop" could as well be reported at the time of injury along with swelling and bruising, impaired grip strength. Sometimes a visible bowstringing of the tendon tin can be seen away from the finger bones if the sheath is completely ruptured. The A2 and A4 pulleys attune force transmission during finger flexion. Therefore, loss of A2 or A4 pulley may result in a permanent, or meaning strength loss.
Preventive measures [edit | edit source]
Here are some guidelines to follow and Lower the risk of rupturing a pulley.
- Open Paw Crimp: Crimping with an open manus will decrease the stress directing on fingers and distribute the force evenly.
- Warm-ups that raises trunk temperature, contracts climbing muscles, move the torso, arms, and hands
- Trunk awareness and paying attending to your body and hand positions on holds and earlier "bearing down"
- Vary handholds later attempting strenuous mitt positions.
- Exist prudent with twisty moves, try to move the torso with the twist instead of all twist into the finger, if possible.
- Kinesio taping
Physiotherapy Management [edit | edit source]
A physiotherapist can help in the diagnosis and treatment of flexor pulley injuries. Handling volition vary depending on the severity of an injury.
By and large, a diagnosis is determined past the following:
- Mechanism of injury: The most likely cause of injury is a fall or slip with a crimp grip sometimes with a respective loud pop at the time of injury. These injuries usually have an acute onset versus overuse.
- Symptoms: Hurting, swelling, bowstringing (seen while multiple pulleys are damaged)
- Imaging: Dynamic Ultrasound is the gold standard for identifying flexor tendon injuries.
The Handling approach for Course I & III Pulley injury: [edit | edit source]
- Relative residuum, icing, and splinting are recommended.
- Finger Extensor Exercises: Overused finger flexors can pb to weakness of the finger extensors, which aid to stabilize fingers while climbing. so it'southward of import to perform finger extensor strengthening exercises to prevent pulley injuries.
- Perform isometric holds at multiple angles to mire the muscle action of a finger while climbing. perform three sets of 30 seconds.
- Taping: After healing, taping tin also be done to provide additional support while climbing.
Post-Operative rehabilitation after flexor tendon pulley repair [edit | edit source]
The goal of the rehabilitation phase process is from hurting, inflammation, and tissue overload stage to achieve full mobility, strength, and somewhen pain-free climbing movement.
Early on-stage [edit | edit source]
The showtime stage of injury is controlling inflammation and it is traditionally done past relative residuum' icing, and taping every bit a form of protection from day to twenty-four hours activities. Climbing is not advisable at this phase.
Rubber-band finger extensions
Hand Strengthening:
- Gripping: Offset using a soft "stress ball", sponge, or easy -rip tool using all fingers and pollex hold, squeeze and the release, later add isometric holds as a progression and so do with a resistance grip tools similar Theraputty.
- Pinching: Working on compression strength is essential for climbing activity. go on thumb and fingers straight, place the ball on the tips of digits, gently squeeze all together, visualizing a tension build upwards in the hand. Also, visualize that having a modest ball in the center of the palm. later progress this exercise using finger springs.
- Condom- Band Finger Extensions: Place an elastic band effectually the PIP joint of fingers and thumb so attempt to open a finger confronting the ring abroad from each other.

Mid-Stage Rehab [edit | edit source]
- Soft-tissue release: Releasing tightened structures like forearm flexors and intrinsic muscles of the paw.
- Weighted Finger Curls: Information technology is besides important to start this do using the first three digits together every bit a warm-up. Later progressing to the private strengthening of an injured finger

- Stretching: stretch fingers and forearm flexor muscles to maintain the elasticity of the muscles.
End-stage Rehab [edit | edit source]
- Finger Board Exercises: Static dead hangs on a fingerboard are a bully way to rehabilitate after early and mid-stage rehab exercises and tests are a pain-free and strong. It is all-time to get-go open-handed, in one case exhausted the possibilities and combinations with open up-handed, endeavour static hangs with half crimp. The safest way to beginning finger/campus board training is, to brainstorm with, anxiety on dead hangs, then hang and reach with feet/foot on, them feet off dead hangs, pull-ups and hang and reach.
- Pull-ups

- Taping: The H-taping method decreased the tendon-bone distance in the injured finger significantly by 16%. the forcefulness development was significantly better with the new tape for the crimp grip position (+13%), merely at that place was no significant improvement for the hanging position. Information technology reduces the tendon-bone distance and provides more stability to pulleys. It is more effective than circular taping. [thirteen]
Render to climbing [edit | edit source]
Criteria and cess examination earlier returning an athlete to climbing needs to be specific to the type of climbing that the patient does, the level, and frequency.
- No hurting with whatever sort of gripping/pinching/crimping with hand tools
- Equal weight of unmarried finger curls for right/left fingers (injured finger and same finger of the other hands, using no more than a v kg weight).
- Pain-complimentary static dead hangs on the fingerboard (start open up-handed then half crimp using front 3 then back 3 in all variation of positions, then front 2 back 2)
- Campusing with good technique if an athlete used to do campusing before an injury. Starting open-handed then with half crimp if they experience its often required. A good composing technique is crucial. It is important to accept a strong cadre, especially obliques, and utilise hips to initiate movements.
- if an athlete returning to difficult bouldering, or hard sport climbing make sure they perform the same, or amend on a fingerboard than have washed in the by.
Collateral ligament strains [edit | edit source]
This type of injury commonly occurs with sideways loadings, such as when throwing one manus out to hold with the other. It well-nigh usually occurs in the PIP joint of the middle finger. Symptoms include pain, swelling, and tenderness effectually an injured finger. Handling for this type of strain is commonly conservative and relative rest, ice, anti-inflammatory medications, and taping the finger for support.
Wrist injuries [edit | edit source]
The most common wrist injury in climbers occurs when there's damage to Triangular fibrocartilage circuitous (TFCC). Information technology provides stability and back up when the paw clenches or the arm rotates. when an athlete feels the onset of wrist pain and continues to climbing pushing through his limits, TFCC tin can go under degenerative and tin even tear. Symptoms include a dull, achy hurting on the side of the wrist and sometimes a throbbing pain is felt when flexing a hand towards the 5th digit. when diagnosed early on, relative rest, anti-inflammatories, and a splint can typically heal this blazon of injury. After healing, taping the wrist while climbing can assist provide additional stability and support to prevent re-injury. In more severe cases, surgery is essential to get rid of the damaged tissue and clean the torn edges; this is also referred to every bit debridement. Recovery from this procedure includes swearing a bandage for several weeks followed by physiotherapy to regain range of motion and strength.
Lower Extremity [edit | edit source]
Traumatic injuries (eg. falls) accounted for eighteen% of injuries and predominantly affecting lower limbs.[14]
Knee injuries [edit | edit source]
Less intuitively, knees are also mutual areas of injury for stone climbers. The repetitive stress from falling during bouldering sessions can easily cause impairment to the meniscus or any of the tendons or ligaments within the articulation. These aforementioned connective tissues are too strained during regular climbing positions if climbers do not have sufficient hip flexibility. Toeing down or edging on pocket-sized holds with hips open and heels raised can crusade abnormal forces exerted on the knees. Drop knees (inward rotation of hip while maintaining leg tension) tin cause a large amount of stress on the knee joint, resulting in injuries as pocket-size as bursitis (inflammation of the bursa) or equally severe as dislocated patella.
Ankle injuries [edit | edit source]
Due to the recurrent falling inherent with climbing (whether during bouldering or roped climbing), ankles are often in danger for sprains and fractures, especially with the soft and flexible shoes used for climbing. Learning proper falling and landing techniques are necessary for the prevention, as well equally careful spotting and belaying of others.
Quick Stats [edit | edit source]
- Injury rates in lower extremities are low and are often caused by trauma.
- Females are more likely to report injuries in the shoulder/arm and more than likely to undergo surgery for injury compared to males.
- A by injury is a significant run a risk gene for re-injury, specially at the site of fingers.
- 51.1% of climbers render to climbing before their injuries are healed, and 44.9% have chronic problems associated with their climbing injury.
Injury Prevention [edit | edit source]
While stone climbing injuries are common, they are not unavoidable. These are steps that peradventure have to reinforce climbing performance and health. Prevention should showtime with educating climbers on the potential adventure for injury. Although adequate rest in betwixt the climbs and reduced grooming them pain is commencement encountered would help in alleviating numerous bug. Early changes in climbing schedules, stretching and exercise habits, and protective taping are necessary to forbid an injury in these climbers.
Warm-Ups [edit | edit source]
Lack of warm-upwards can increment the likelihood of an injury. A thorough warm-upwards increases blood flow, musculus flexibility, and body control and it will actuate all of the essential muscling used for the climbing activity. A 2022 study of handball players (Andersson et al.) showed that a comprehensive warm-up program tin can decrease injury rates past up to 28&. A%complete warm-up includes four components, all to exist performed in the post-obit sequence:
- Increase blood flow
- Meliorate Mobility
- Stability exercises
- proprioception
1. Increase blood flow with aerobic exercises for 5-10 minutes to elevate deep-muscle temperature, which makes the muscles more adaptable and lessen the risk of strain or tear
2. Amend mobility with dynamic stretching and it's proven to be the all-time choice. Research supports that a sport-specific dynamic warm-up is the all-time way to increase blood flow to the muscles and tendons in the body. This method prepares the body for a selected activity and may help reduce injury rates.
Dynamic warm-ups include:
- On The Wall
Uses the entire trunk to generate warmth. It mirrors specific trunk positions that are used while climbing.
How to practice:Flex your hip upwardly towards the chest. grab knees and pull to towards the breast and and then release back down to the floor.
- Rotation
Uses rotational movements to warm-up the muscles. This often-disregarded phase and information technology's extremely important in climbing due to the rotational nature of the sport.
- Arms
Uses dynamic stretching to warm a primary muscle information technology's opposing muscle during a single motion.
- Wrist and Fingers
Targets the smaller muscle groups with tendon glides.
[15]
3. Target stability with musculus-activation exercises:
For injury prevention train antagonist muscles of fingers and wrist extensors, shoulder rotators, and scapular muscles along with dynamic stretches which give a foundation for injury-costless climbing experience. Grooming antagonist muscles tin improve posture and reduces hurting.

Ecentric triceps extensions
- Strengthening exercises includes-
Isometric bent over T, Eccentric triceps extension, Core grooming, Hanging superhighway ups, Pull ups, Plank knee-to-Elbow etc.
[16]
- Weight training: includes single-leg heel raise, Shoulder press, Bulgarian split squats, etc.
4. Proprioception training for stability can be performed including exercises like:
- Human foot Stabbing:
Stand on the ground, about an inch away from the climbing wall. Make sure there are depression pes Chips to use. Slowly begin leaning forward until getting to the tipping point and experience similar falling over. Immediately stick a human foot out to any of the foot fries on the wall to catch yourself. Target how close the foot was to landing correct on acme of the foot chip. It'southward difficult to consistently get the pes in proper position on the hold.
- Blinking:
Try this as you lot climb upward or downwardly a route. Equally an athlete climbing, cheque the next foothold. Before moving the foot to that hold, then try endmost eyes all the way until the foot is on the new hold. Repeat this for each foot hold-ups route. So try to progress it past doing with the hands
- Brainstorm climbing with a gradual increment in route difficulty. Begin climbing with a gradual increase in route difficulty.
References [edit | edit source]
- ↑ Cole, Keegan P. MD; Uhl, Richard L. Doctor; Rosenbaum, Andrew J. Md Comprehensive Review of Rock Climbing Injuries, Journal of the American Academy of Orthopaedic Surgeons: June 15, 2022 - Volume 28 - Result 12 - p e501-e509 doi: 10.5435/JAAOS-D-19-00575
- ↑ Jones One thousand, Johnson MI. A critical review of the incidence and risk factors for finger injuries in rock climbing. Electric current sports medicine reports. 2022 Nov 1;15(half dozen):400-ix.
- ↑ Neuhof A, Hennig FF, Schöffl I, Schöffl 5. Injury risk evaluation in sport climbing. International journal of sports medicine. 2022 Oct;32(ten):794-800
- ↑ Holtzhausen LM, Noakes TD. Elbow, forearm, wrist, and hand injuries amongst sport stone climbers.Clin J Sport Med. 1996;six(3):196-203. doi:x.1097/00042752-199607000-00010
- ↑ Mugleston B, McMullen C. Musculoskeletal Injuries in Climbers. Current Physical Medicine and Rehabilitation Reports. 2022 Sep 15;7(3):179-85.
- ↑ Chang CY, Torriani M, Huang AJ. Rock climbing injuries: acute and chronic repetitive trauma. Electric current problems in diagnostic radiology. 2022 May 1;45(iii):205-14.
- ↑ Lutter C, Schweizer A, Hochholzer T, Bayer T, Schöffl V. Pulling harder than the hamate tolerates: evaluation of hamate injuries in rock climbing and bouldering. Wilderness & environmental medicine. 2022 Dec 1;27(4):492-9.
- ↑ Desaldeleer Equally, Le Nen D. Bilateral fracture of the base of operations of the middle phalanx in a climber: Literature review and a case written report. Orthopaedics & Traumatology: Surgery & Research. 2022 May 1;102(iii):409-11.
- ↑ Jones, Gareth PhDane; Schöffl, Volker PhDi,2,3,4; Johnson, Mark I. PhD1 Incidence, Diagnosis, and Management of Injury in Sport Climbing and Bouldering: A Disquisitional Review, Current Sports Medicine Reports: November 2022 - Volume 17 - Issue 11 - p 396-401 doi: 10.1249/JSR.0000000000000534
- ↑ Roseborrough A, Lebec M. Differences in static scapular position between rock climbers and a non-rock climber population. North American journal of sports physical therapy: NAJSPT. 2007 Feb;2(1):44.
- ↑ Simon Thousand, Popp D, Lutter C, Schöffl V. Functional and sports-specific outcome after surgical repair of rotator gage tears in rock climbers. Wilderness & Environmental Medicine. 2022 December 1;28(iv):342-7.
- ↑ Robert Pedowitz, Christine B. Chung, Donald Resnick,Magnetic Resonance Imaging in Orthopedic Sports Medicine,google books, 2008
- ↑ Schöffl I, Einwag F, Strecker W, Hennig F, Schöffl V. Impact of taping after finger flexor tendon caster ruptures in rock climbers. Journal of practical biomechanics. 2007 Feb ane;23(1):52-62.
- ↑ Maitland 1000. Injuries associated with rock climbing.J Orthop Sports Phys Ther. 1992;sixteen(2):68-73. doi:10.2519/jospt.1992.sixteen.two.68
- ↑ Dynamic climbing Warm-upwardly Available from: https://youtu.be/B86QxHCDiM0
- ↑ Rock climbing fitness tests- Hanging pike, 2 Rep Pull Up, and twenty mm Edge Dead-Hang Available from: https://youtu.be/hCkJEM2L3j0

Source: https://www.physio-pedia.com/Rock_Climbing_Injuries
Posted by: smiththerhatim.blogspot.com
0 Response to "How To Prevent Re Injury Of A Jones Fracture Surgical Repair"
Post a Comment